
Unraveling Esophageal Varices: A Nurse’s Guide to a Critical Condition and Effective Esophageal varices nursing care
In the world of gastroenterology and critical care, few conditions present as abruptly and dramatically as a ruptured esophageal varix. One moment, your patient may be stable, and the next, you’re managing a life-threatening hemorrhage. Understanding the “why” behind esophageal varices and the “how” of nursing care is crucial for any nurse.
This guide will break down the pathophysiology, signs, management, and—most importantly—provide a detailed nursing care plan to help you confidently manage patients with this high-stakes condition.
Essential Techniques for Effective Esophageal Varices Nursing Care
Implementing effective Esophageal varices nursing care is essential for improving patient outcomes.
What Are Esophageal Varices? (And Why Are They So Dangerous?)
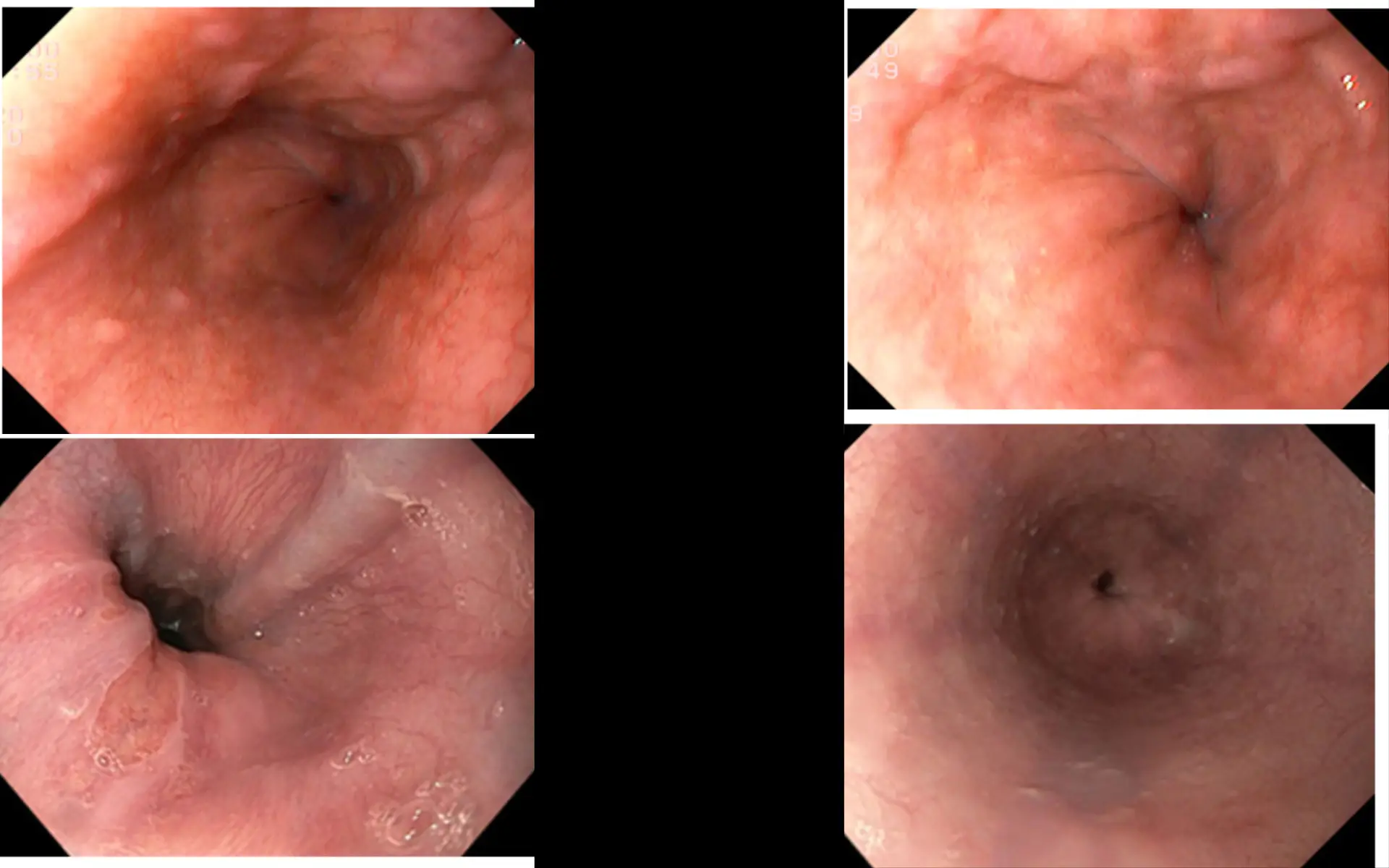
Think of esophageal varices as varicose veins, but in the worst possible place: the esophagus. They are abnormally enlarged, swollen veins at the lower end of the esophagus.
The root cause is almost always portal hypertension. Here’s the simple breakdown: Do Yoga Click Here
- The Liver as a Filter: The portal vein brings blood from the digestive organs (stomach, intestines, spleen) to the liver to be filtered.
- The Roadblock: In conditions like liver cirrhosis (the most common cause), scar tissue blocks the normal flow of blood through the liver.
- The Traffic Jam: This blockage causes a massive pressure backup in the portal vein system—this is portal hypertension.
- The Detour: The blood, desperate to return to the heart, seeks alternative routes. It diverts through smaller, fragile veins that aren’t designed to handle this high pressure, primarily in the esophagus, stomach, and rectum.
- The Rupture Risk: These new pathways (varices) become engorged and thin-walled. A simple increase in pressure—from coughing, vomiting, or even straining—can cause them to rupture, leading to catastrophic bleeding.
![A simple diagram showing the liver, portal vein, and esophageal varices would be ideal here in a real blog post.]
Signs and Symptoms of Esophageal Varices : The Silent Threat and the Loud Emergency
Esophageal varices often have a dual nature: they can be completely asymptomatic until they bleed.
Signs of Unruptured Varices (Often signs of underlying liver disease):
- Jaundice (yellowing of skin and eyes)
- Ascites (fluid buildup in the abdomen)
- Spider angiomas
- Easily bruising or bleeding
- Hepatic encephalopathy (confusion, lethargy)
Signs of a Ruptured Varix (A MEDICAL EMERGENCY):
- Hematemesis: Vomiting large amounts of bright red blood. This is the classic, terrifying sign.
- Melena: Black, tarry, foul-smelling stools (from digested blood).
- Hematochezia: Passing bright red blood from the rectum (occurs with massive, rapid bleeding).
- Signs of Hypovolemic Shock:
- Hypotension (low blood pressure)
- Tachycardia (rapid heart rate)
- Pallor (pale skin), cool, clammy skin
- Altered mental status (confusion, dizziness, loss of consciousness)
- Decreased urine output. Increase Your Mental Power
Medical Management: Stabilize, Stop the Bleed, and Prevent Recurrence
Management is a multi-pronged attack focused on immediate stabilization and definitive treatment.
- Emergency Stabilization (The ABCs):
- Airway: Protect the airway! Massive hematemesis poses a huge aspiration risk. The patient may require intubation.
- Breathing: Administer supplemental oxygen.
- Circulation:
- Establish two large-bore IVs (16-18 gauge) immediately.
- Aggressive fluid resuscitation with crystalloids (Normal Saline, Lactated Ringer’s).
- Administer blood products: packed red blood cells (PRBCs), fresh frozen plasma (FFP) to correct coagulopathy, and platelets.
- Pharmacologic Intervention:
- Octreotide (Sandostatin): A somatostatin analog that reduces splanchnic blood flow and portal pressure. It’s a first-line drug for active variceal bleeding.
- Vasopressin: A potent vasoconstrictor, but used less frequently now due to significant side effects (e.g., cardiac ischemia).
- Proton Pump Inhibitors (PPIs): IV pantoprazole to prevent stress ulcers and reduce risk of re-bleeding.
- Antibiotics: Prophylactic antibiotics (e.g., ceftriaxone) are often given as active bleeding increases the risk of bacterial infections.
- Definitive Treatment:
- Endoscopy (EGD): The gold standard for both diagnosis and treatment.
- Endoscopic Variceal Ligation (EVL) or “Banding”: A small elastic band is placed around the varix, cutting off its blood supply. This is the preferred method.
- Sclerotherapy: A sclerosing agent is injected into the vein to cause it to clot and collapse.
- Balloon Tamponade (Sengstaken-Blakemore Tube): A temporary, last-resort measure if endoscopy fails. A tube with two balloons (one gastric, one esophageal) is inserted to apply direct pressure to the bleeding sites. This is a critical care procedure with high risks, including esophageal rupture and airway obstruction.
- TIPS (Transjugular Intrahepatic Portosystemic Shunt): A radiologist creates a shunt within the liver to bypass the scarred tissue, directly connecting the portal vein to the hepatic vein. This effectively reduces portal pressure but can worsen hepatic encephalopathy.
- Endoscopy (EGD): The gold standard for both diagnosis and treatment.
Nursing Care Plan for Esophageal Varices (Active Bleed)
A patient with a bleeding esophageal varix is one of the sickest patients you will encounter. Your role is pivotal in stabilization and preventing further decline. Here are the priority nursing diagnoses and interventions.
Priority Nursing Diagnosis #1: Deficient Fluid Volume & Ineffective Tissue Perfusion
- Related to: Active hemorrhage from ruptured esophageal varices.
- As Evidenced By: Hematemesis, melena, hypotension, tachycardia, decreased urine output, pallor.
Goal: The patient will achieve hemodynamic stability and maintain adequate tissue perfusion.
| Nursing Interventions | Rationale |
| Monitor vital signs (BP, HR, RR, O2 sat) every 15 minutes or more frequently as indicated. | Frequent monitoring is essential to detect signs of hypovolemic shock and evaluate the patient’s response to interventions. |
| Establish and maintain at least two large-bore IV catheters (16-18 gauge). | Large-bore access is critical for rapid administration of fluids, blood products, and medications. |
| Administer IV fluids (crystalloids) and blood products (PRBCs, FFP, platelets) as ordered. | Replaces lost volume, improves oxygen-carrying capacity (RBCs), and corrects clotting factor deficiencies (FFP) to help stop bleeding. |
| Monitor hemoglobin, hematocrit, and coagulation studies (PT/INR). | Provides objective data on the extent of blood loss and the effectiveness of transfusions and clotting factor replacement. |
| Insert an indwelling urinary catheter and monitor output hourly. | Urine output is a sensitive indicator of renal perfusion and overall fluid status. Less than 30 mL/hr is a critical finding. |
| Assess for signs of ongoing bleeding (continued hematemesis, melena) and worsening shock (declining BP, altered LOC). | Early recognition of treatment failure allows for rapid escalation of care (e.g., preparing for balloon tamponade or TIPS). |
Priority Nursing Diagnosis #2: Ineffective Airway Clearance & Risk for Aspiration
- Related to: Active vomiting of blood and potential for altered level of consciousness.
- As Evidenced By: Hematemesis, gurgling sounds, dyspnea, decreased oxygen saturation.
Goal: The patient will maintain a patent airway and be free from signs of aspiration. Health Mantra Watch
| Nursing Interventions | Rationale |
| Position the patient in a semi-Fowler’s or side-lying position if not contraindicated. | Promotes drainage of secretions and vomitus from the mouth, reducing the risk of aspiration into the lungs. |
| Keep suction equipment readily available at the bedside. Use a Yankauer suction catheter as needed. | Allows for immediate clearance of the oropharynx to maintain airway patency during an episode of vomiting. |
| Monitor respiratory rate, rhythm, depth, and oxygen saturation continuously. Auscultate lung sounds frequently. | Tachypnea, desaturation, and new adventitious sounds (crackles, rhonchi) can indicate aspiration has occurred. |
| Maintain NPO status. | Prevents further oral intake that could increase vomiting and aspiration risk. Prepares the patient for an emergent endoscopy. |
| Assess level of consciousness (LOC) and gag reflex. Be prepared for emergent intubation. | A declining LOC or loss of a gag reflex significantly increases aspiration risk. The healthcare team may elect to intubate to protect the airway. |
Priority Nursing Diagnosis #3: Anxiety & Fear
- Related to: Life-threatening situation (hemorrhage), invasive procedures, and fear of death.
- As Evidenced By: Restlessness, verbalization of fear, increased heart rate, panicked expression.
Goal: The patient will report a reduction in anxiety and demonstrate effective coping mechanisms.
| Nursing Interventions | Rationale |
| Maintain a calm, confident, and reassuring demeanor while providing care. | Your calmness can be contagious and help reduce the patient’s and family’s anxiety. It builds trust in a crisis. Click Here Yoga |
| Explain all procedures and interventions in simple, clear terms, even if the patient’s LOC is altered. | Reduces fear of the unknown. Even sedated or confused patients may be able to hear and understand, which can be comforting. |
| Acknowledge the patient’s fear. Use therapeutic communication techniques like, “This must be very frightening for you.” | Validating the patient’s feelings helps build a therapeutic relationship and shows empathy. |
| Keep the patient and family informed of the plan of care as much as possible. | Involving them in the care process can provide a sense of control and reduce feelings of powerlessness. |
| Administer sedative medications as ordered, carefully monitoring for respiratory depression. | Judicious use of anxiolytics can help manage severe anxiety, which can exacerbate tachycardia and hypertension. Know More: |
Caring for a patient with bleeding esophageal varices is a true test of nursing skill, blending critical thinking, rapid intervention, and compassionate care. By understanding the underlying pathophysiology and prioritizing the ABCs, you can act as a stabilizing force in a chaotic situation. Your meticulous monitoring, timely interventions, and calming presence are not just tasks on a care plan—they are the lifeline for your patient in their most vulnerable moment. Health Mantra Watch
Disclaimer: For Informational Purposes Only
This information is intended for general educational purposes and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read here.