
Crohn’s Disease: Overview and Nursing Care Plan:
Introduction of Crohn’s Disease:
Crohn’s Disease is a chronic inflammatory bowel disease (IBD) that affects the gastrointestinal (GI) tract.
It can occur anywhere from the mouth to the anus, but most commonly involves the terminal ileum and colon.
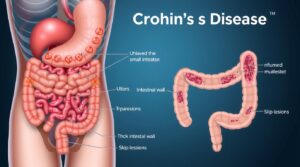
The disease is characterized by inflammation that extends through all layers of the bowel wall, leading to ulceration, scarring, and narrowing of the intestinal lumen.
Crohn’s Disease is progressive and relapsing, meaning it alternates between periods of flare-ups and remission. There is currently no known cure, but symptoms can be effectively managed through medication, diet, and lifestyle adjustments.
Definition of Crohn’s Disease :
Crohn’s Disease is a chronic, inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal (GI) tract from the mouth to the anus, but most commonly involves the small intestine (ileum) and the colon. It is characterized by inflammation that extends through all layers of the bowel wall (transmural inflammation) and often appears in patches or skip lesions, with healthy tissue interspersed between inflamed areas. Unlike ulcerative colitis, which primarily affects the large intestine and only the innermost lining, Crohn’s can lead to strictures, fistulas, and abscesses due to its deep, patchy inflammation.
Etiology and Pathophysiology of Crohn’s Disease :
The exact cause of Crohn’s disease is unknown, but it is believed to be a multifactorial condition resulting from a complex interplay of:
-
Genetic Predisposition: A family history of IBD increases risk. Numerous gene mutations have been identified (e.g., NOD2/CARD15), which may affect the immune response or gut barrier function.
-
Immune System Dysfunction: The immune system mistakenly attacks harmless bacteria, food, or even the bowel tissue itself, leading to chronic inflammation. It’s an overactive and misdirected immune response.
-
Environmental Factors:
-
Smoking: A significant risk factor, worsening the disease course and increasing the need for surgery.
-
Diet: While diet doesn’t cause Crohn’s, certain foods can trigger symptoms in individuals. High intake of processed foods, refined sugars, and low fiber may contribute to inflammation.
-
Medications: NSAIDs can exacerbate symptoms. Oral contraceptives may have a slight association.
-
Infections: Exposure to certain bacteria or viruses may trigger an immune response in genetically susceptible individuals.
-
Gut Microbiota: Imbalance in the gut bacteria (dysbiosis) is thought to play a crucial role.
-
Pathophysiology of Crohn’s Disease :
In Crohn’s Disease, the immune system mistakenly attacks healthy intestinal tissue, leading to chronic inflammation.
This results in:
-
Thickening of the intestinal wall.
-
Formation of ulcers, fistulas, and strictures.
-
Malabsorption due to damaged mucosa.
Lesions are discontinuous (“skip lesions”), meaning normal segments of intestine alternate with diseased areas — a hallmark feature distinguishing it from ulcerative colitis.
Diagnostic Studies of Crohn’s Disease :
-
Blood Tests:
-
CBC: Anemia (low Hgb/Hct), leukocytosis (elevated WBC during acute inflammation/infection).
-
ESR/CRP: Elevated markers of inflammation.
-
Electrolytes: May be abnormal due to diarrhea/vomiting.
-
Albumin: Low levels indicate malnutrition.
-
Vitamin levels: B12, D, Iron studies.
-
Stool Studies: Rule out infections (C. diff, pathogens). Fecal calprotectin or lactoferrin (markers of intestinal inflammation).
-
Antibodies: ANCA (atypical perinuclear anti-neutrophil cytoplasmic antibodies) and ASCA (anti-Saccharomyces cerevisiae antibodies) can help differentiate IBD types, but are not definitive.
-
-
Endoscopic Procedures with Biopsy (Gold Standard):
-
Colonoscopy with Ileoscopy: Visualizes the colon and terminal ileum, allowing for direct observation of inflammation, ulcers, strictures, and collection of biopsies. Biopsies confirm transmural inflammation and granulomas (a characteristic finding, though not always present).
-
Upper Endoscopy: Used if upper GI symptoms are present.
-
Capsule Endoscopy: A swallowed camera pill to visualize the entire small bowel, especially useful for areas not reached by traditional endoscopy.
-
-
Imaging Studies:
-
CT Enterography/MR Enterography: Specialized CT/MRI scans that visualize the entire small bowel and colon to assess inflammation, strictures, fistulas, and abscesses. Considered superior to traditional barium studies.
-
Abdominal X-rays: To check for obstruction or toxic megacolon (rare in Crohn’s).
-
Barium Studies (Upper GI series with small bowel follow-through): Less common now, but can show “string sign” (narrowed lumen), skip lesions, and mucosal irregularities.
-
Ultrasound: Can sometimes identify thickened bowel wall or abscesses.
-
Signs and Symptoms of Crohn’s Disease :
Common symptoms include:
-
Persistent diarrhea (may be bloody or watery)
-
Abdominal pain and cramping (often in the right lower quadrant)
-
Weight loss and fatigue
-
Fever and malaise during flare-ups
-
Mouth ulcers
-
Rectal bleeding
-
Nutritional deficiencies (e.g., vitamin B12, iron, protein)
Complications may include:
-
Intestinal obstruction
-
Fistula formation (abnormal connections between bowel and other organs)
-
Abscesses
-
Colon cancer (long-term risk)
Treatment of Crohn’s Disease :
Treatment aims to achieve and maintain remission, improve quality of life, prevent complications, and avoid surgery. It is highly individualized.
-
Pharmacological Therapy:
-
Aminosalicylates (5-ASAs): Mesalamine (Asacol, Lialda, Pentasa) – typically for mild-to-moderate disease, less effective for Crohn’s than UC.
-
Corticosteroids: Prednisone, Budesonide (Entocort) – used for acute flares to rapidly reduce inflammation. Not for long-term use due to side effects (osteoporosis, hyperglycemia, infection risk). Budesonide has fewer systemic side effects as it acts locally.
-
Immunomodulators: Azathioprine (Imuran), 6-mercaptopurine (6-MP), Methotrexate – suppress the immune system long-term to maintain remission and reduce steroid dependence. Slow onset of action (weeks to months).
-
Biologic Therapies (Anti-TNF, Anti-Integrin, Anti-IL-12/23): Infliximab (Remicade), Adalimumab (Humira), Ustekinumab (Stelara), Vedolizumab (Entyvio) – target specific inflammatory pathways. Used for moderate-to-severe disease not responsive to other therapies. High efficacy but also higher cost and potential for serious side effects (e.g., infection, malignancy).
-
Antibiotics: Metronidazole, Ciprofloxacin – used for perianal disease, abscesses, or bacterial overgrowth.
-
-
Nutritional Therapy:
-
Dietary Modifications: No universal “Crohn’s diet.” Patients often identify trigger foods (e.g., high-fiber, spicy, fatty foods, dairy, caffeine). Low-residue diet during flares.
-
Nutritional Supplements: Ensure adequate caloric and protein intake. Vitamin B12, D, iron, calcium supplementation as needed.
-
Enteral/Parenteral Nutrition: May be necessary in severe cases for bowel rest, to correct malnutrition, or for those with short bowel syndrome.
-
-
Surgical Intervention:
-
Surgery is not curative for Crohn’s but often necessary for complications.
-
Indications: Strictures causing obstruction, fistulas unresponsive to medical therapy, abscesses, severe perianal disease, toxic megacolon (rare), massive hemorrhage.
-
Common Procedures:
-
Resection: Removal of diseased bowel segments, with rejoining of healthy ends (anastomosis).
-
Stricturoplasty: Widening of narrowed segments of bowel without resection.
-
Fistulotomy/Seton Placement: For complex fistulas.
-
Ostomy: In severe cases, a temporary or permanent ileostomy or colostomy may be required.
-
-
Nursing Care Plan (NCP) of Crohn’s Disease :
| Nursing Diagnosis | Goals / Expected Outcomes | Nursing Interventions | Rationales | Evaluation |
| 1. Diarrhea related to bowel inflammation and mucosal irritation | – Patient will experience reduced frequency of diarrhea. – Patient will maintain adequate hydration. |
1. Monitor stool frequency, color, and consistency. 2. Record intake and output accurately. 3. Encourage low-residue, high-protein diet. 4. Administer antidiarrheal and anti-inflammatory medications as prescribed. 5. Provide access to bathroom facilities and maintain hygiene. |
1. Evaluates disease activity and fluid loss. 2. Ensures accurate assessment of fluid balance. 3. Reduces bowel stimulation and promotes healing. 4. Controls inflammation and decreases intestinal motility. 5. Promotes comfort and prevents skin breakdown. |
– Frequency of bowel movements reduced. – Patient remains hydrated with moist mucous membranes and stable vitals. |
| 2. Imbalanced Nutrition: Less than body requirements related to malabsorption and decreased intake | – Patient will maintain or gain weight within normal range. – Patient will demonstrate knowledge of dietary modifications. |
1. Assess dietary habits and nutritional intake. 2. Provide small, frequent, nutrient-rich meals. 3. Collaborate with dietitian for individualized plan. 4. Administer vitamin and mineral supplements as ordered. 5. Monitor lab values (albumin, hemoglobin, electrolytes). |
1. Identifies deficiencies and eating patterns. 2. Promotes better nutrient absorption and tolerance. 3. Ensures balanced, patient-specific nutrition. 4. Prevents or corrects nutritional deficiencies. 5. Evaluates effectiveness of nutritional therapy. |
– Patient’s weight stabilized or improved. – Laboratory values within normal range. |
| 3. Acute Pain related to intestinal inflammation and cramping | – Patient will report relief from pain (≤3/10 on pain scale). – Patient will appear relaxed and participate in care. |
1. Assess pain intensity, location, and triggers. 2. Administer prescribed analgesics and antispasmodics. 3. Encourage relaxation techniques (deep breathing, guided imagery). 4. Provide rest periods and cluster nursing care. 5. Use heat application if appropriate (warm compress). |
1. Provides baseline for evaluating treatment response. 2. Relieves pain and reduces bowel spasms. 3. Reduces stress and muscle tension, which can worsen pain. 4. Prevents fatigue and promotes comfort. 5. Improves circulation and relieves discomfort. |
– Patient reports decreased pain. – Patient able to rest and perform ADLs comfortably. |
| 4. Risk for Deficient Fluid Volume related to excessive diarrhea and decreased intake | – Patient will maintain adequate fluid balance (urine output ≥30 mL/hr, normal skin turgor). | 1. Monitor vital signs and daily weight. 2. Assess for signs of dehydration (dry mucosa, poor skin turgor). 3. Encourage oral fluids; provide IV fluids if needed. 4. Record fluid intake and output. 5. Monitor electrolyte levels (Na+, K+, Cl–). |
1. Detects early signs of fluid deficit. 2. Evaluates hydration status. 3. Restores fluid balance and prevents hypovolemia. 4. Tracks hydration progress accurately. 5. Identifies imbalances requiring correction. |
– Patient’s hydration status remains stable. – No signs of dehydration observed. |
| 5. Anxiety related to chronic illness, lifestyle changes, and fear of recurrence | – Patient will verbalize reduced anxiety. – Patient will express feelings and participate in care decisions. |
1. Assess level of anxiety and coping mechanisms. 2. Provide emotional support and active listening. 3. Encourage expression of fears and concerns. 4. Educate patient about disease process and treatment. 5. Refer to counseling or support groups if needed. |
1. Establishes baseline and guides interventions. 2. Builds trust and therapeutic relationship. 3. Helps patient process emotions constructively. 4. Increases knowledge, which reduces uncertainty. 5. Promotes psychological well-being. |
– Patient reports decreased anxiety. – Actively participates in care and demonstrates understanding of illness. |
| 6. Knowledge Deficit related to lack of information about disease and self-care | – Patient will demonstrate understanding of Crohn’s Disease, treatment plan, and dietary needs. | 1. Assess patient’s baseline knowledge and readiness to learn. 2. Provide clear, written, and verbal education about medications, diet, and symptom monitoring. 3. Teach importance of medication adherence and follow-up visits. 4. Encourage stress management and smoking cessation. 5. Involve family in education for support. |
1. Identifies learning needs and barriers. 2. Reinforces key points to enhance understanding. 3. Improves compliance and disease control. 4. Prevents flare-ups and promotes overall health. 5. Builds a strong support system for patient adherence. |
– Patient verbalizes and demonstrates correct self-care practices. – Reports adherence to medications and diet. |
🧠 Summary
This nursing care plan focuses on managing symptoms, preventing complications, promoting adequate nutrition and hydration, and supporting the emotional well-being of patients with Crohn’s Disease.
Effective nursing care combines clinical observation, patient education, and compassionate support to enhance quality of life and promote long-term disease control.
Disclaimer:
This blog is for informational and educational purposes only. The images included are AI-generated illustrations and may not represent real individuals, equipment, or medical settings.