
Small Intestinal Bacterial Overgrowth (SIBO): Overview & Nursing Care Plan |
Introduction of Small Intestinal Bacterial Overgrowth (SIBO):
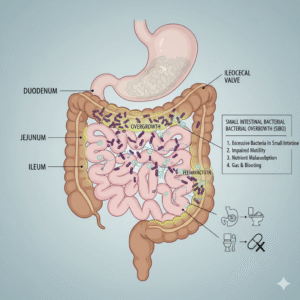
Small Intestinal Bacterial Overgrowth (SIBO) is a condition characterized by an excessive amount of bacteria in the small intestine, which should normally have relatively few bacteria compared to the large intestine. This overgrowth can lead to a variety of gastrointestinal symptoms and malabsorption issues.
Causes/Risk Factors of Small Intestinal Bacterial Overgrowth (SIBO):
-
Impaired Motility: Conditions that slow down the movement of food through the small intestine, such as gastroparesis, scleroderma, or opioid use.
-
Structural Abnormalities: Anatomical issues like strictures, fistulas, diverticula, or surgical alterations (e.g., gastric bypass, blind loops) that create stagnant areas where bacteria can proliferate.
-
Reduced Gastric Acid: Chronic use of proton pump inhibitors (PPIs) or conditions like atrophic gastritis reduce stomach acid, allowing more bacteria to survive and reach the small intestine.
-
Pancreatic Insufficiency: Insufficient pancreatic enzymes can lead to undigested food in the small intestine, providing a substrate for bacterial growth.
-
Immunodeficiency: Weakened immune systems may be less effective at clearing bacteria.
-
Ileocecal Valve Dysfunction: A compromised ileocecal valve allows bacteria from the colon to reflux into the small intestine.
-
Celiac Disease/Crohn’s Disease: These inflammatory conditions can alter motility and intestinal architecture.
-
Diabetes: Autonomic neuropathy associated with diabetes can impair intestinal motility.
Pathophysiology of Small Intestinal Bacterial Overgrowth (SIBO):
Signs and Symptoms:
-
Bloating and Abdominal Distension: Often worsening after meals.
-
Abdominal Pain/Cramping:
-
Diarrhea: Steatorrhea (fatty stools) due to malabsorption.
-
Constipation: More common in methane-dominant SIBO.
-
Excessive Gas/Flatulence:
-
Nausea:
-
Unexplained Weight Loss: Due to malabsorption.
-
Nutrient Deficiencies: Especially B12, fat-soluble vitamins (A, D, E, K), and iron.
-
Fatigue:
-
Skin Rashes (e.g., rosacea): Some associations have been noted.
The small intestine is designed for nutrient absorption, and its natural defenses (such as gastric acid, intestinal motility, and the ileocecal valve) usually prevent bacterial overgrowth. However, when these defenses are impaired, bacteria from the large intestine can colonize the small intestine. These bacteria ferment carbohydrates, producing gases (hydrogen, methane, hydrogen sulfide) that cause bloating and discomfort. They also deconjugate bile acids, impairing fat digestion and absorption, and consume nutrients like vitamin B12, leading to deficiencies.
Signs and Symptoms of Small Intestinal Bacterial Overgrowth (SIBO):
-
Bloating and Abdominal Distension: Often worsening after meals.
-
Abdominal Pain/Cramping:
-
Diarrhea: Steatorrhea (fatty stools) due to malabsorption.
-
Constipation: More common in methane-dominant SIBO.
-
Excessive Gas/Flatulence:
-
Nausea:
-
Unexplained Weight Loss: Due to malabsorption.
-
Nutrient Deficiencies: Especially B12, fat-soluble vitamins (A, D, E, K), and iron.
-
Fatigue:
-
Skin Rashes (e.g., rosacea): Some associations have been noted.
Diagnosis of Small Intestinal Bacterial Overgrowth (SIBO):
-
Hydrogen/Methane Breath Test: The most common diagnostic tool. Patients ingest a sugar (lactulose or glucose), and the exhaled breath is measured for hydrogen and methane gases produced by bacteria. An early rise in these gases indicates SIBO.
-
Small Bowel Aspirate and Culture: Considered the “gold standard” but is invasive. A sample of fluid from the small intestine is collected during endoscopy and cultured for bacterial count.
-
Response to Antibiotic Therapy: Sometimes, a trial of antibiotics is used; symptom improvement can suggest SIBO.
Treatment of Small Intestinal Bacterial Overgrowth (SIBO):
-
Antibiotics: Rifaximin is commonly used, as it has a targeted effect in the small intestine and is poorly absorbed systemically. Other antibiotics may be used depending on the suspected bacterial type.
-
Prokinetics: Medications to improve intestinal motility.
-
Dietary Modifications:
-
Low-FODMAP Diet: Restricting fermentable carbohydrates that feed bacteria.
-
Elemental Diet: A liquid diet with pre-digested nutrients, giving the gut a rest.
-
Specific Carbohydrate Diet (SCD): Similar to low-FODMAP, focusing on easily digestible carbohydrates.
-
-
Addressing Underlying Causes: Treating the primary condition contributing to SIBO (e.g., correcting structural abnormalities, managing motility disorders).
-
Nutritional Support: Supplementing deficient vitamins and minerals.
-
Lifestyle Changes: Stress management, regular exercise.
Nursing Care Plan for Small Intestinal Bacterial Overgrowth (SIBO):
I. Nursing Diagnosis: Imbalanced Nutrition: Less Than Body Requirements related to malabsorption and altered digestive processes secondary to SIBO.
-
Expected Outcomes:
-
Patient will maintain current weight or demonstrate weight gain towards ideal body weight.
-
Patient will report improved energy levels.
-
Patient will exhibit normal laboratory values (e.g., albumin, prealbumin, iron, B12, fat-soluble vitamins).
-
Patient will verbalize understanding of dietary modifications to optimize nutrient intake.
-
-
Nursing Interventions:
-
Assess Nutritional Status:
-
Monitor weight, BMI, and anthropometric measurements regularly.
-
Assess dietary intake, noting types and quantities of food consumed, and symptoms associated with specific foods.
-
Review laboratory results (e.g., CBC, electrolytes, albumin, prealbumin, B12, vitamin D).
-
Observe for signs of nutrient deficiencies (e.g., glossitis, cheilosis, peripheral neuropathy, brittle nails).
-
-
Collaborate with Dietitian:
-
Facilitate consultation with a registered dietitian for individualized dietary counseling, including low-FODMAP, elemental, or SCD diets as prescribed.
-
Educate patient on reading food labels and identifying trigger foods.
-
-
Provide Nutritional Support:
-
Administer prescribed vitamin and mineral supplements (e.g., B12 injections, fat-soluble vitamins) as ordered.
-
Suggest small, frequent meals rather than large ones to reduce digestive burden.
-
Encourage consumption of easily digestible foods as tolerated.
-
Discuss potential benefits and proper use of digestive enzymes if indicated.
-
-
Patient Education:
-
Explain the importance of adhering to prescribed dietary changes and antibiotic regimen.
-
Teach patient to keep a food and symptom diary to identify individual triggers.
-
Provide resources for SIBO-friendly recipes and meal planning.
-
-
II. Nursing Diagnosis: Acute Pain related to abdominal distension, cramping, and excessive gas production secondary to bacterial fermentation.
-
Expected Outcomes:
-
Patient will report a decrease in pain intensity to a manageable level (e.g., ≤3/10 on a pain scale).
-
Patient will demonstrate use of non-pharmacological pain relief methods.
-
Patient will verbalize understanding of factors that exacerbate pain.
-
-
Nursing Interventions:
-
Assess Pain:
-
Utilize a pain scale (e.g., 0-10) to assess pain intensity, location, quality, and duration.
-
Assess aggravating and alleviating factors.
-
Observe for non-verbal cues of pain (e.g., grimacing, guarding, restlessness).
-
-
Administer Pharmacological Interventions:
-
Administer prescribed analgesics or antispasmodics as ordered, evaluating their effectiveness.
-
Educate patient on the proper use and potential side effects of medications.
-
-
Implement Non-Pharmacological Interventions:
-
Encourage application of warm compresses to the abdomen.
-
Teach relaxation techniques (e.g., deep breathing, guided imagery, meditation).
-
Encourage gentle ambulation as tolerated to promote gas expulsion.
-
Suggest wearing loose-fitting clothing to avoid abdominal compression.
-
Recommend peppermint oil capsules (enteric-coated) if appropriate and approved by the healthcare provider.
-
-
Patient Education:
-
Instruct patient on dietary modifications that can reduce gas production (e.g., avoiding carbonated beverages, chewing food thoroughly, eating slowly).
-
Explain the role of antibiotics in reducing bacterial load and subsequently pain.
-
Encourage regular bowel habits to reduce discomfort.
-
-
III. Nursing Diagnosis: Diarrhea or Constipation related to altered gut microbiome, malabsorption, and motility disturbances.
-
Expected Outcomes:
-
Patient will report improved bowel regularity and consistency.
-
Patient will demonstrate fluid and electrolyte balance.
-
Patient will verbalize understanding of interventions to manage altered bowel patterns.
-
-
Nursing Interventions:
-
Assess Bowel Habits:
-
Monitor frequency, consistency, color, and odor of stools.
-
Assess for presence of steatorrhea (fatty, foul-smelling stools that float).
-
Assess for signs of dehydration (e.g., dry mucous membranes, decreased skin turgor, orthostatic hypotension) in cases of diarrhea.
-
Assess for abdominal distension and discomfort in cases of constipation.
-
-
Promote Fluid and Electrolyte Balance (for Diarrhea):
-
Encourage increased oral fluid intake (water, clear broths, electrolyte solutions).
-
Administer intravenous fluids if indicated and ordered.
-
Monitor electrolyte levels (e.g., potassium, sodium).
-
-
Manage Constipation (for Methane-Dominant SIBO):
-
Encourage adequate fiber intake from tolerated sources (as directed by dietitian).
-
Promote regular physical activity to stimulate bowel motility.
-
Administer prescribed laxatives or stool softeners if ordered, cautiously, as motility agents are sometimes contraindicated in specific SIBO cases without careful consideration.
-
Ensure adequate fluid intake.
-
-
Medication Management:
-
Administer prescribed antibiotics as ordered, educating patient on the importance of completing the full course.
-
Discuss the use of prokinetic agents to improve motility if prescribed.
-
-
Patient Education:
-
Instruct patient on dietary changes that can help regulate bowel movements (e.g., identifying and avoiding trigger foods for diarrhea, increasing tolerated fiber for constipation).
-
Emphasize the importance of hydration.
-
Teach proper perianal care for diarrhea to prevent skin breakdown.
-
-
IV. Nursing Diagnosis: Deficient Knowledge regarding SIBO diagnosis, treatment, and self-management strategies.
-
Expected Outcomes:
-
Patient will verbalize accurate understanding of SIBO and its causes.
-
Patient will correctly explain the prescribed treatment plan, including medication regimen and dietary restrictions.
-
Patient will identify strategies for managing symptoms and preventing recurrence.
-
-
Nursing Interventions:
-
Assess Knowledge Level:
-
Ask the patient what they know about SIBO and their current treatment plan.
-
Identify any misconceptions or gaps in understanding.
-
-
Provide Comprehensive Education:
-
Explain SIBO in clear, understandable terms, including its pathophysiology, common symptoms, and diagnostic process.
-
Detail the prescribed antibiotic regimen: name, dosage, frequency, duration, and potential side effects. Emphasize compliance.
-
Thoroughly review dietary recommendations (e.g., low-FODMAP, SCD), providing written materials and practical tips.
-
Explain the importance of addressing underlying causes of SIBO.
-
Discuss potential complications of untreated SIBO (e.g., nutrient deficiencies, weight loss).
-
-
Reinforce Self-Management Strategies:
-
Teach symptom monitoring and when to report worsening symptoms or new concerns to the healthcare provider.
-
Discuss the importance of follow-up appointments and repeat breath testing if indicated.
-
Provide information on lifestyle modifications, such as stress management techniques and regular exercise.
-
Offer resources for support groups or reliable online information.
-
-
Encourage Questions and Clarification:
-
Use the “teach-back” method to ensure the patient understands the information provided.
-
Create a supportive environment for the patient to ask questions.
-
-
V. Nursing Diagnosis: Risk for Ineffective Health Maintenance related to complexity of treatment regimen, chronic nature of SIBO, and potential for recurrence.
-
Expected Outcomes:
-
Patient will verbalize commitment to long-term management strategies.
-
Patient will demonstrate ability to integrate SIBO management into daily life.
-
Patient will adhere to follow-up appointments and screenings.
-
-
Nursing Interventions:
-
Identify Barriers to Adherence:
-
Discuss with the patient any perceived difficulties in following dietary restrictions, medication schedules, or lifestyle changes (e.g., financial constraints, social pressures, lack of support).
-
Assess the patient’s motivation and readiness for change.
-
-
Facilitate Support Systems:
-
Involve family members or significant others in education and care planning if appropriate and with patient consent.
-
Refer to support groups or counseling services if needed.
-
-
Provide Practical Solutions:
-
Help the patient develop realistic meal plans and shopping lists.
-
Suggest strategies for managing SIBO while dining out or traveling.
-
Discuss medication reminders (e.g., alarms, pill organizers).
-
-
Emphasize Long-Term Perspective:
-
Educate the patient that SIBO can be a recurrent condition and ongoing vigilance and management are often necessary.
-
Encourage a proactive approach to symptom management and early intervention if symptoms return.
-
Reinforce the importance of a strong patient-provider relationship for ongoing care.
-
-
Remember, this is a general care plan, and individual patient needs will vary. Always tailor the care plan to the specific presentation, comorbidities, and preferences of the patient.
Disclaimer:
This blog is for informational and educational purposes only. The images included are AI-generated illustrations and may not represent real individuals, equipment, or medical settings.